

When Being a "Good Mom" Feels Like a Prison: The Hidden Face of Postpartum OCD
You love your baby more than anything—but what if your desire to protect them has started stealing your peace? Postpartum OCD often hides behind “good motherhood,” convincing moms that one more precaution, one more check, or one more reassurance will finally create safety. Learn why OCD is really a struggle with uncertainty—and how ERP therapy helps moms reclaim their confidence.
By Dr. Erin Cook, PsyD, PMH-C | Red Elm Psychotherapy
It's 3:00 AM and your baby is finally asleep. Instead of resting, you're awake on Amazon comparing medical-grade sanitizing wipes for stroller wheels. You've already washed the pacifier four times tonight, your hands sting from the harsh soap, and your mind keeps whispering: “Just a few more steps and my baby will be safe.”
The next day, you tentatively mention your exhaustion to another mom. She smiles sympathetically and says, "Honestly, you can never be too careful these days. You're just such a good mom."
And suddenly, instead of recognizing how miserable you are, society accidentally reinforces the very clinical anxiety that is keeping you trapped.
How Anxiety Hides Behind "Good" Motherhood
One of the hardest parts about postpartum OCD (Obsessive-Compulsive Disorder) is that it constantly hides behind behaviors our culture celebrates. We praise mothers for sacrificing their sleep, admire moms who are endlessly vigilant, and celebrate the parent who has researched every chemical, anticipated every danger, and stayed one step ahead of every possible threat.
Our culture has created a difficult equation: we often celebrate constant hypervigilance as the mark of a devoted mother. It's easy to start believing that if you could just be careful enough, you could prevent every bad outcome.
Because of this cultural camouflage, it can be incredibly difficult to recognize when a healthy protective instinct has crossed the line into a clinical issue.
Imagine an adult without children washing every doorknob in their home fifty times a day because they're terrified of contamination. Most people would immediately recognize that as a sign of OCD. Now imagine a brand-new mother disinfecting every bottle, throwing away food because it might have touched a "dirty" counter, or spending hours tracking ambient air quality.
People call her responsible. Careful. Protective. Meanwhile, she is quietly unraveling inside.
The Trap of Postpartum Contamination OCD: Moving the Goalposts
Postpartum OCD has an exhausting way of convincing you that just one more precaution will finally grant you peace of mind. It tells you safety is just around the corner if you do:
One more Google search about infant illness.
One more boiling sterilization cycle for the pump parts.
One more frantic portal message to your pediatrician.
One more reassurance-seeking question to your partner.
But the relief never lasts. Within minutes, your brain finds another terrifying possibility, another looming uncertainty, or another microscopic threat you should have anticipated.
That is because OCD doesn't actually care about safety—it demands absolute certainty. And absolute certainty does not exist when you are raising a living, breathing human being in an unpredictable world.
Why Perinatal OCD Hijacks Your Best Instincts
"I just want to be a good mom and keep my baby safe."
In our Vienna, VA psychotherapy practice, this is the exact sentence Niles and I hear most often from suffering mothers. They don't want perfect floors or pristine houses; they want to protect their child.
That is what makes perinatal OCD so heartbreaking. It hijacks the most beautiful, fierce, instinctive part of being a parent—your desire to protect your baby—and slowly turns it into a psychological prison. Underneath your exhausting rituals isn't irrationality; there is profound love.
But OCD quietly adds one devastating, false assumption to that love: If something bad ever happens, it means you didn't do enough.
Good Parenting is Not Risk Elimination
Every parent makes hundreds of choices a day that involve inherent risk. We buckle our children into car seats—not because they make driving 100% safe, but because they make it safer. We hold their hand crossing a parking lot, knowing we still can't control every distracted driver.
Good parenting has never been about achieving zero risk. It is about making thoughtful decisions while accepting that some uncertainty remains.
There is no magical checklist that guarantees a child will never get sick. No amount of obsessive cleaning eliminates every environmental risk. OCD treats this natural human uncertainty like an emergency that must be solved right now, promising you that if you just wash longer or research harder, you'll finally earn the peace you long for.
The goalpost will always move.
Because the goal of motherhood isn't becoming certain.
The goal of motherhood is learning to love deeply in a world where certainty doesn't exist.
You were never meant to carry the impossible responsibility of guaranteeing your child's safety. No parent can.
What ERP Therapy Actually Looks Like at Red Elm Psychotherapy
Many moms avoid reaching out for help because they are terrified of what treatment entails. They worry a therapist is going to force them to stop caring about germs altogether, or command them to be "gross" or reckless with their baby.
As specialized ERP clinicians, we want you to know: That is not what treatment looks like.
Exposure and Response Prevention (ERP), the gold-standard evidence-based treatment for OCD, isn't about becoming careless. It doesn't ask you to ignore legitimate pediatric health recommendations. Instead, it helps you build the skills to notice when anxiety—not your actual parenting values—is calling the shots.
Healthy caution asks:
"Have I taken reasonable, common-sense steps to care for my baby?"Postpartum OCD asks:
"But how can I be 100% absolutely sure there isn't a single germ left?"
ERP helps you learn to recognize the difference.
ERP helps you tell the difference. Recovery isn't about caring less about your child. It's about no longer confusing certainty with love.

Putting Down the Shield
Think of your postpartum anxiety like carrying a massive, heavy iron shield. At first, it made perfect sense to pick it up. Of course you want to protect your newborn.
But over time, OCD convinces you that you can never set that shield down. You sleep with it. You eat with it. You end up holding your baby awkwardly with one arm because your other arm is always white-knuckled, gripping the heavy shield. Eventually, the very tool meant to protect your family becomes the weight that keeps you from fully living.
ERP therapy doesn't ask you to abandon your child's safety. It simply helps you put the shield down when anxiety—not actual danger—is demanding you carry it. Because when your hands aren't occupied by fear, they are finally free to hold your baby, to rest, and to notice the beautiful moments that OCD has been stealing from you.
Postpartum OCD Therapy in Vienna, Virginia & Across PSYPACT States
If your "good mom" habits have started to feel like a prison, you do not have to keep carrying this weight alone.
At Red Elm Psychotherapy, we specialize in helping mothers recover from the exhausting cycles of postpartum OCD and perinatal anxiety using evidence-based, compassionate ERP. We provide specialized, non-judgmental care tailored to the unique pressures of motherhood.
We offer in-person therapy sessions at our office in Vienna, Virginia, as well as convenient virtual teletherapy across Virginia and multiple states via PSYPACT.
Recovery isn't about becoming a less careful mother—it’s about becoming a free one. Let's work together to help you put down the shield and start enjoying your baby again.

Face Your Fears, Change Your Brain: What to Expect in ERP Therapy for OCD
ERP therapy can sound scary: “Wait…you want me to face the thing I’m most afraid of?”
But ERP isn’t about forcing yourself to be fearless. It’s about learning that anxiety, uncertainty, and intrusive thoughts don’t have to control your life.
In our newest blog, we walk through what ERP therapy actually looks like—from understanding your OCD cycle to practicing new ways of responding.
If you’re struggling with OCD, intrusive thoughts, or perinatal OCD, you’re not alone.
If you’re searching for ERP therapy for OCD in Virginia, you may already know what it feels like to be stuck in the OCD cycle.
A thought shows up.
Your anxiety spikes.
Your brain tells you that you need to figure it out, prevent something bad from happening, or get reassurance before you can move on.
Maybe you find yourself:
Asking others for reassurance again and again
Avoiding situations that feel unsafe
Mentally reviewing conversations, memories, or decisions
Trying to “cancel out” intrusive thoughts
Checking until something finally feels right
These strategies make sense. They are your brain’s attempt to protect you.
The problem is that OCD learns from what you do next. Every time you respond to anxiety with a compulsion, your brain gets the message:
"This thought must have been important. I needed to do something to feel safe."
Over time, the cycle becomes stronger.
Exposure and Response Prevention (ERP) therapy helps your brain learn a different message:
"I can experience uncertainty. I can feel anxiety. I can have an intrusive thought—and I do not have to respond to it."
At Red Elm Psychotherapy, we specialize in ERP therapy for OCD, intrusive thoughts, and perinatal OCD, serving clients across Virginia and through PSYPACT telehealth.
What Is ERP Therapy for OCD?
Exposure and Response Prevention (ERP) is a specialized form of cognitive behavioral therapy designed specifically to treat OCD.
The name can sound intimidating. Many people hear “exposure” and imagine being forced to face their biggest fear immediately.
That is not what good ERP looks like.
ERP is a collaborative process where you and your therapist identify the patterns that keep OCD going and gradually practice responding differently.
The goal is not to eliminate anxiety forever.
The goal is to stop letting anxiety and OCD make your decisions for you.
ERP involves two parts:
Exposure: Gently and intentionally approaching thoughts, situations, sensations, or uncertainties that OCD tells you to avoid.
Response Prevention: Practicing not engaging in compulsions that temporarily reduce anxiety but keep OCD stuck over time.
What Happens in ERP Therapy?
Understanding Your OCD Cycle
Before starting ERP, your therapist will help you understand how OCD is keeping you stuck.
Together, you’ll look at the thoughts or fears that trigger anxiety and the things you do afterward to try to feel safe or certain.
For many people, those responses are not obvious. They may look like checking, asking for reassurance, avoiding situations, or spending hours trying to analyze a thought until it finally feels resolved.
The problem is that OCD keeps moving the finish line. No amount of checking, analyzing, or reassurance can create the complete certainty OCD is demanding.
ERP helps you begin stepping out of that cycle.Creating a Personalized Exposure Plan
ERP does not mean walking into your biggest fear on the first day of therapy.
Instead, you and your therapist create a gradual plan for practicing uncertainty. This might include approaching situations you have been avoiding, allowing uncomfortable thoughts to be present, or practicing not engaging in the rituals that OCD demands.
The objective is to help you discover that you can experience discomfort and still safely move forward
Learning to Respond Differently
This is the heart of ERP.
When OCD shows up, it often creates a sense of urgency:
"You need to figure this out right now."
"You need to make sure."
"You cannot move on until you feel certain."
ERP helps you practice a different response.
Instead of:
"How do I make this anxiety go away?"
you learn:
"Can I allow this feeling to be here while continuing with my life?"
This might mean resisting the urge to check, avoiding reassurance seeking, or allowing an intrusive thought to exist without trying to analyze what it means.
Over time, your brain learns that anxiety is uncomfortable—but it is not an emergency.
What Changes With ERP?
Over time, many people notice that OCD begins to take up less space.
You may find yourself:
Spending less time analyzing and seeking reassurance
Feeling less controlled by intrusive thoughts
Making decisions based on your values instead of fear
Anxiety and fear can come up, but they no longer make the rules.
ERP Therapy for Perinatal OCD: When Intrusive Thoughts Feel Terrifying
Perinatal OCD can show up as frightening intrusive thoughts, intense guilt, repeated reassurance seeking, or avoiding situations that feel risky. Many mothers find themselves caught in a cycle of trying to prove they are safe, responsible, and "good enough"-but the search for certainty never quite ends.
A Perinatal OCD Example
Many mothers with perinatal OCD describe an experience like this:
After the birth of her baby, a mother begins experiencing intrusive thoughts about something terrible happening. The thoughts feel vivid, unwanted, and deeply upsetting.
She starts wondering:
"What if this thought means something? What if I can't trust myself?"
She begins avoiding situations that trigger anxiety, asking her partner for reassurance, and mentally reviewing moments to figure out whether she missed something.
What makes ERP feel so difficult is not just the anxiety.
It is the feeling that not responding to the thoughts would be irresponsible.
"If there is even a small chance something could happen, shouldn't I do everything I can to prevent it?"
This fear is one reason perinatal OCD can feel so convincing.
Mothers are often surrounded by messages that they should anticipate every possible danger, prevent every mistake, and always know the right thing to do. OCD can take that understandable desire to protect and turn it into an impossible demand for certainty.
In ERP, the goal is not to prove that nothing bad could ever happen.
Instead, therapy focuses on learning that intrusive thoughts are not warnings or commands.
For example, an exposure might involve allowing an intrusive thought to be present during a normal parenting activity while practicing not engaging in compulsions that keep OCD going—such as reassurance seeking, mental reviewing, or avoidance.
The goal is not to become careless.
The goal is to learn that you can be a caring, responsible mother without needing absolute certainty before you trust yourself.
Over time, many mothers find that the thoughts become less urgent, and they are able to spend more time being present with their babies instead of constantly trying to prevent imagined dangers.
This is a fictional example created to illustrate how perinatal OCD can show up and how ERP therapy works.
ERP Therapy in Virginia and Through PSYPACT Telehealth
Finding specialized OCD treatment can be challenging. Many therapists are trained in general anxiety treatment but do not have specific training in ERP.
At Red Elm Psychotherapy, we provide:
OCD therapy in Vienna, VA
ERP therapy for OCD in Northern Virginia
Virtual ERP therapy across participating PSYPACT states
Specialized treatment for perinatal OCD and intrusive thoughts
You do not have to spend years trying to outthink OCD.
Start ERP Therapy for OCD in Virginia
If you are struggling with OCD, intrusive thoughts, or perinatal OCD, therapy can help you break free from the cycle of fear and compulsions.
Starting ERP can feel intimidating—but you do not have to feel completely ready before reaching out.
Many people begin therapy feeling unsure, scared, or convinced their thoughts are different from everyone else’s.
You are not the first person to bring these fears into therapy.
At Red Elm Psychotherapy, we provide compassionate, specialized ERP therapy for OCD across Virginia and through PSYPACT telehealth.
Schedule a consultation to learn how ERP therapy can help you move toward a life that is guided by your values—not by OCD.

How to Find an OCD Specialist in Northern Virginia (And Why Specialization Matters)
Not all therapy approaches treat OCD effectively. Learn why Exposure and Response Prevention (ER) is considered the gold- standard treatment, how to find an OCD specialist in Northern Virginia, and what questions to ask when choosing a therapost. We also discuss why specialized care is especially important during pregnancy and postpartum.
If you’ve been in therapy before and still feel like OCD is running your life, you’re not alone.
Many people with OCD spend months—or even years—in therapy before receiving treatment that actually targets OCD. They may leave sessions feeling understood and supported, yet still find themselves trapped in the same exhausting cycle of intrusive thoughts, compulsions, reassurance-seeking, and self-doubt.
That doesn’t mean therapy can’t help.
It usually means you haven’t been given the right treatment for OCD.
At Red Elm Psychotherapy, we specialize in treating OCD using Exposure and Response Prevention (ERP), the gold-standard treatment for OCD. We often meet clients across Northern Virginia who tell us, “I’ve been in therapy for years, but no one ever explained OCD this way.”
Why General Therapy Isn’t Always Enough for OCD
Standard therapy tools are incredibly valuable.
Supportive therapy can help people navigate grief, relationship challenges, work stress, trauma, depression, and major life transitions. Many compassionate therapists provide exceptional care using these approaches.
But OCD works differently.
Imagine breaking your arm. Your primary care physician is highly trained and incredibly knowledgeable—but they’re still likely to refer you to an orthopedic surgeon. Not because your primary care doctor isn’t good at their job, but because certain conditions require specialized expertise.
OCD is much the same.
OCD is driven by a cycle of intrusive thoughts, anxiety, compulsions, and temporary relief. Because of how this cycle works, some therapy strategies that are helpful for other concerns can unintentionally strengthen OCD.
For example, spending time analyzing why you had a particular thought, searching for certainty, or repeatedly offering reassurance can actually reinforce OCD’s message that the thought is dangerous and must be solved.
It’s not that those therapy approaches are “wrong.”
It’s that OCD requires a different blueprint.
Why Exposure and Response Prevention (ERP) Works
ERP is considered the gold-standard treatment for OCD because it targets the cycle that keeps OCD alive.
Rather than trying to convince you that your intrusive thoughts aren’t true, ERP teaches your brain something much more powerful:
You can experience uncertainty, anxiety, or intrusive thoughts—and choose not to respond with compulsions.
That might mean resisting mental checking, avoiding reassurance, postponing Google searches, stopping confession rituals, or gradually approaching situations OCD has taught you to fear.
Over time, your brain begins to learn that anxiety naturally rises and falls without needing compulsions to make it disappear.
This process helps retrain your brain’s alarm system. Instead of learning, “I survived because I checked,” your brain begins learning, “I survived because I didn’t need to check.”
Research consistently shows that ERP changes the way the brain responds to intrusive thoughts in a way that simply talking about the anxiety cannot.
Effective ERP Should Be Evidence-Based and Human
Many people come to us after trying ERP elsewhere with mixed experiences.
Some describe treatment that felt incredibly rigid—sessions focused almost exclusively on anxiety ratings, or feeling as though every question was met with silence out of fear that any response might become reassurance. Others leave believing ERP means being pushed into overwhelming exposures before they feel understood.
That isn’t how we practice.
At Red Elm Psychotherapy, ERP is the foundation of our OCD treatment because it’s the most effective, evidence-based approach we have. But we also believe that healing happens within a strong therapeutic relationship.
That means we take time to understand your story, teach you how OCD works, and collaborate on exposures that are challenging without being overwhelming. We integrate cognitive behavioral strategies and an attachment-informed understanding of relationships while keeping ERP at the center of treatment.
Our goal isn’t to withhold warmth or become emotionally distant. It’s to avoid reinforcing OCD while helping you feel genuinely supported.
You should never have to choose between evidence-based treatment and a therapist who feels human.
What This Looks Like in Real Life
(Note: To protect client confidentiality, the following scenario is a composite case study reflecting common patterns seen in our practice.)
One client came to us after several years of therapy for anxiety. She was thoughtful, self-aware, and had done a lot of work to understand her thoughts. On the surface, it seemed like she “should” have been feeling better by that point.
But her OCD hadn’t changed.
She was still spending hours each day mentally reviewing conversations, trying to determine whether she had said or done something “wrong.” She sought reassurance from loved ones, experienced brief relief, and then quickly found herself back in doubt. Much of her prior therapy had focused on understanding why she felt anxious and processing the distress, which helped her feel supported—but didn’t change the underlying cycle.
When we began ERP, the focus shifted. Instead of trying to solve or analyze the thoughts, she practiced allowing them to be present without engaging in the mental review or reassurance-seeking that followed.
At first, this felt unfamiliar and uncomfortable. Her OCD consistently pushed her toward “figuring it out” the way she always had.
But over time, something important changed: the thoughts didn’t disappear, but they also didn’t pull her into hours of rumination. The urgency softened. The cycle began to lose momentum.
What she described later wasn’t a life without intrusive thoughts—it was a life where she no longer felt trapped in them.
That shift is often what recovery from OCD looks like.
Why Specialized OCD Care Matters Even More During Pregnancy and Postpartum
While finding an OCD specialist is important for anyone with OCD, it becomes especially important during pregnancy and the postpartum period.
Perinatal OCD often involves intrusive thoughts about accidentally or intentionally harming the baby. These thoughts can feel terrifying, especially when they seem completely out of character.
One of the biggest fears we hear from new mothers is: “What if someone thinks these thoughts mean I want to hurt my baby?”
The good news is that intrusive thoughts are actually incredibly common during the perinatal period. For someone with OCD, these thoughts are ego-dystonic—meaning they are unwanted, deeply distressing, and completely inconsistent with who you are as a parent.
Unfortunately, providers without specialized training in perinatal OCD may mistake these symptoms for postpartum anxiety alone, respond with repeated reassurance, or, in rare cases, misunderstand them as postpartum psychosis.
These are very different conditions requiring different treatment approaches.
An OCD specialist understands these differences and knows that ERP can safely and effectively treat perinatal OCD while supporting the unique realities of pregnancy and early parenthood.
The goal isn’t to convince you that you’ll never have another intrusive thought.
The goal is to help those thoughts lose their power, so you can spend more time connecting with your baby and less time trapped in fear.
Questions to Ask When Looking for an OCD Therapist in Northern Virginia
Not every therapist specializes in OCD—and that’s okay. Just like in medicine, different clinicians develop expertise in different areas.
If you’re looking for OCD treatment in Northern Virginia (including Vienna, Mclean, Fairfax, Arlington, or Loudoun County), consider asking potential providers:
What percentage of your practice is dedicated to treating OCD?
Have you received specialized training in Exposure and Response Prevention (ERP)?
What does a typical ERP session look like?
How do you respond when clients seek reassurance during sessions?
Do you regularly treat the specific type of OCD I’m experiencing, such as postpartum OCD, scrupulosity, health OCD, or relationship OCD?
These questions can help you determine whether a therapist has the experience needed to provide evidence-based OCD treatment.
You Don’t Have to Stay Stuck
Living with OCD can be exhausting, but it is also highly treatable.
If you’ve tried therapy before without lasting relief, that doesn’t mean you’ve failed therapy. It may simply mean you haven’t yet received treatment specifically designed for OCD.
At Red Elm Psychotherapy, we provide evidence-based ERP for adults through in-person therapy at our Vienna, VA office and via telehealth throughout the state of Virginia. We also specialize in treating perinatal OCD, helping parents navigate pregnancy and postpartum with compassionate, expert care.
Recovery doesn’t require getting rid of every intrusive thought. It comes from learning that you no longer have to listen to them.
Ready to Take the Next Step?
If you're ready to break the OCD cycle, we are here to walk with you. Click here to schedule a free 15-minute consultation with us today.

Why Reassurance Seeking Feels Necessary When You Have OCD—and Why It Quietly Makes Things Worse
If you find yourself repeatedly asking for reassurance, checking, or searching for certainty, it may feel like the only way to feel calm. In OCD, that relief is real—but temporary, and it often keeps the cycle going.
When you’ve been drowning in anxiety, reassurance can start to feel like the only lifeline. Asking a partner if everything is okay. Checking in with a doctor “just to be sure.” Going over a memory again because something about it feels off. Searching online for answers that might finally settle the uncertainty.
The relief that comes right after someone tells you “you’re okay” can feel like the only moment in the day when your nervous system fully drops. For a brief stretch of time, things feel settled. The thought softens. The body calms. The urgency fades.
But OCD doesn’t resolve through reassurance. And so the doubt returns—often quietly at first, then with more intensity. What makes this so confusing is that reassurance does work, just not in the way it seems. It reduces anxiety temporarily, but over time it also strengthens the cycle that brings the anxiety back.
In OCD, reassurance doesn’t function as connection or clarity. It functions as relief. And relief, in this case, becomes part of what keeps the loop going.
The Core Mechanism: The Trap of Immediate Relief
What makes reassurance so compelling is how quickly it works. There’s often a brief window where everything feels resolved, even if nothing has actually changed. And that brief relief is powerful enough that the brain starts to learn something very specific: that uncertainty needs to be fixed immediately, and that feeling better depends on getting certainty before moving forward.
So when the doubt returns—as it always does—it often feels more convincing, not less.
If reassurance worked in the way people hope it does, why does the anxiety come back so quickly? Why does the same question return in slightly different forms, again and again? And why does it feel harder to let go of the thought each time it shows up?
The answer is that reassurance teaches the brain to treat uncertainty as something urgent. Each time you seek an answer or chase an absolute, the mind learns that the thought was important enough to stop everything for. Over time, that reinforces the idea that you cannot move forward until you feel completely sure. Instead of calming the system, this process quietly trains it to produce more doubt—a classic hallmark of the OCD cycle.
The Invisible Forms of Reassurance
Reassurance in OCD rarely stays obvious. It expands and becomes harder to recognize over time, shifting from external questions into quieter, internal mental habits.
Sometimes it shows up as replaying situations over and over in your mind, trying to figure out whether something “felt right” or whether you missed something important.
Other times it looks like monitoring your internal reactions—checking whether you feel the “correct” amount of guilt, certainty, or concern about a thought.
It can also show up in comparison loops, where you measure your reactions against how you imagine other people would respond, as a way of making sense of your own experience.
Or it becomes information-seeking that never fully resolves anything, where reading and rereading eventually stops feeling clarifying and starts feeling like part of the loop itself.
These internal forms of reassurance are especially hard to notice because they don’t look like compulsions from the outside. But the function is the same: trying to eliminate uncertainty through repeated checking, analysis, or review.
The Conscientiousness Trap (and the Need for Control)
For many people, this process becomes exhausting without them fully realizing why. It can feel like constant problem-solving that never actually reaches a conclusion. The mind keeps generating new angles, new “what ifs,” and new questions, each one feeling like it needs to be addressed before you can move on.
This pattern is especially common in people who are thoughtful, responsible, and deeply attuned to doing things correctly.
The same conscientiousness that helps someone be careful or ethical can also make uncertainty harder to tolerate. If something matters, it makes sense to want to be sure. OCD can take that same conscientiousness and turn it into something that never feels finished.
At its core, this is an attempt to create certainty in an inherently uncertain world. If you can be careful enough, responsible enough, or thorough enough, the mind begins to believe that it can prevent bad outcomes. Because of this, reassurance seeking can blend into everyday behavior in ways that are incredibly easy to miss.
In high-achieving adults, it can look like over-preparing, over-checking, or looping through decisions long after they’ve been made. For example, someone might find themselves asking 10 to 15 people for input on a simple decision—not because they actually need more information, but because each new perspective briefly quiets the feeling that something might be wrong or incomplete.
In relationships, it can show up as needing repeated confirmation about feelings, intentions, or how interactions were perceived. For example, someone experiencing symptoms of Relationship OCD (ROCD) might feel an urgent need to review a routine text conversation with a partner or friend, asking for reassurance that they didn’t come across the wrong way, even long after the interaction is over.
In parents, it often shows up as repeated checking in about whether a child is truly okay, whether a minor situation was handled perfectly, or whether some vague but feared harm was missed—closely tying into the loops often seen in perinatal and postpartum OCD.
The Relational Ripple Effect
Over time, these patterns don’t just stay within the individual. They begin to shape the relational environment around them. Partners, family members, or even colleagues can become part of the reassurance cycle, offering well-meaning responses that reduce distress in the moment but unintentionally keep the pattern going.
When this happens, the system itself can begin to organize around managing anxiety rather than tolerating uncertainty. This is part of why OCD can feel so persistent—it is often reinforced not just internally, but interpersonally as well.
Changing Your Relationship to Uncertainty
Treatment, especially Exposure and Response Prevention (ERP), works differently. It does not aim to create perfect certainty or eliminate doubt. Instead, it focuses on changing your relationship to uncertainty so that it no longer requires immediate resolution.
This often means practicing the hardest part: not asking the question, not checking again, not reviewing the memory, and not waiting for the feeling of certainty to arrive before moving forward. At first, this can feel completely counterintuitive because it goes against everything the mind has learned about how to feel safe. But over time, allowing the discomfort to rise and fall on its own begins to weaken the belief that uncertainty is an emergency.
The goal isn’t to stop caring or stop checking in on what matters. It’s to stop needing certainty as a prerequisite for living. OCD tends to demand certainty first—but recovery is learning how to move forward without letting that demand take the lead.
If you are feeling stuck in an exhausting loop of anxiety and reassurance seeking, you don't have to navigate it alone. Reach out to Red Elm Psychotherapy to connect with an OCD specialist in Virginia today.
Is It Perfectionism, or Is It "Just Right" OCD?
"For a long time, your attention to detail may have felt like one of your greatest strengths. But somewhere along the way, what once felt helpful started feeling exhausting. If your brain won’t let you move on until a task, an email, or a space feels 'just right,' you aren't just a perfectionist—and you aren't alone. Here is how to break the loop."
For a long time, your attention to detail may have felt like one of your greatest strengths.
You were the person who caught mistakes other people missed. The person who cared deeply. The person who stayed up a little later, worked a little harder, and pushed things a little further.
Maybe those qualities helped you succeed in school, build a career, care for your family, or create a life you're proud of.
But somewhere along the way, what once felt helpful started feeling exhausting.
You spend twenty minutes writing an email that should take two.
You can't stop thinking about a conversation from yesterday because something about it still feels unsettled.
You reorganize the same space over and over, searching for a feeling of completion that never quite arrives.
You tell yourself, "Just finish it and move on."
But your brain won't let you.
When "Doing Your Best" Stops Feeling Like a Choice
Many people assume OCD is always about contamination fears or checking behaviors. But for some people, OCD shows up as an overwhelming need for things to feel right.
Not perfect in the traditional sense.
Just right.
It can feel like an internal tension, a sense that something is unfinished, uneven, incomplete, or off.
You may not be worried that something terrible will happen if you leave it alone.
The problem is that leaving it alone can feel almost physically uncomfortable.
So you rewrite.
You reread.
You replay.
You rearrange.
You try one more time.
And then one more.
Not because you want to—but because you're desperately trying to get rid of that uncomfortable feeling.
The Part That People Don't See
From the outside, people often assume you're organized, conscientious, or highly motivated.
What they don't see is how much energy the OCD cycle takes.
The mental loops.
The second-guessing.
The way simple tasks can consume enormous amounts of time.
The frustration of knowing you're capable of more but feeling stuck in endless revisions and re-doing.
Many of the professionals and parents we work with describe feeling trapped between two realities:
Part of them knows they're spending too much time on something.
Another part feels completely unable to stop.
That tug-of-war can be exhausting.
Why the Relief Never Lasts
The difficult thing about chasing the "just right" feeling is that it rarely stays.
Maybe you finally send the email.
Maybe you finally organize the room.
Maybe you finally find the exact wording you've been searching for.
There's a brief sense of relief.
And then your brain starts looking for the next thing that's off.
The next thing that needs adjusting.
The next thing that doesn't quite feel complete.
Over time, life can start to shrink around those moments.
Not because you're lazy.
Not because you're incapable.
But because so much energy is going toward managing discomfort.
Learning to Live With "Good Enough"
One of the hardest truths about "Just Right" OCD is that the goal isn't to make everything feel right.
The goal is learning that you can tolerate the feeling when it doesn't.
That might mean sending the email before it feels finished.
Leaving the picture frame slightly crooked.
Walking away from a task when it's good enough.
Not because you don't care.
Because your life is bigger than the pursuit of certainty, completeness, or perfect alignment.
Through Exposure and Response Prevention (ERP), people gradually learn something surprising:
The discomfort doesn't last forever.
And they don't have to keep obeying it.
When You're Ready for More Freedom
If you're exhausted by the constant revising, rethinking, redoing, or striving for a feeling that never quite arrives, you're not alone.
Many high-achieving professionals and parents find themselves caught in these patterns.
The good news is that change doesn't require lowering your standards or becoming someone who doesn't care.
It means learning how to care deeply about your work, your family, and your values without being controlled by the need for everything to feel exactly right.
f you're looking for support in Northern Virginia, specialized OCD therapy can help you step off the treadmill. Reach out to our Vienna, VA office to connect with Niles Cook, PsyD today and reclaim your time, energy, and peace of mind.
Prefer to meet online? While we love seeing clients face-to-face in our Vienna office, we also provide specialized online OCD therapy and ERP services virtually across Virginia and all PSYPACT-participating states.
About the Author
Dr. Niles Cook is a clinical psychologist specializing in OCD and anxiety disorders, with advanced training in Exposure and Response Prevention. At Red Elm Psychotherapy, he helps adults across Virginia understand their OCD cycle, reduce compulsions, and build a more flexible relationship with fear, doubt, and uncertainty.
Trying to Conceive Without Losing Yourself: Understanding Fertility Anxiety and OCD
For many women, the emotional journey into parenthood begins long before a positive pregnancy test. When the path to pregnancy becomes consumed by an exhausting cycle of anxiety, hyper-tracking, and a search for certainty, you aren't just stressed—your mind may be caught in an OCD loop. Learn how to carry hope without losing yourself in the process.
For many women, becoming pregnant isn't as straightforward as they imagined.
After years of preventing pregnancy, it can be startling to discover how much uncertainty is involved in trying to conceive (TTC). What many expected to be a simple next step can instead become months or years of planning, medical appointments, fertility treatments, disappointments, and difficult waiting.
For some women, the emotional journey into parenthood begins long before a positive pregnancy test.
Feeling anxious during this process is completely understandable. When something matters deeply, uncertainty naturally feels difficult. But sometimes anxiety becomes more than worry. Thoughts become "sticky." Reassurance never seems to last. Tracking starts to consume more and more time.
For some individuals, the struggle is not just fertility-related stress. It is anxiety or OCD attaching itself to fertility and reproduction.
When Anxiety Becomes a Full-Time Job
Many women experiencing fertility-focused anxiety appear thoughtful, informed, and responsible from the outside. They know the details of their cycle. They have researched treatment options. They are paying close attention to their health.
But internally, they may feel trapped in a cycle of fear and vigilance, constantly wondering:
What if my body is broken?
What if I waited too long?
What if something I did years ago affected my fertility?
What if I missed my fertile window?
What if this symptom means something important?
What if I never become a parent?
These thoughts often feel urgent, important, and impossible to ignore.
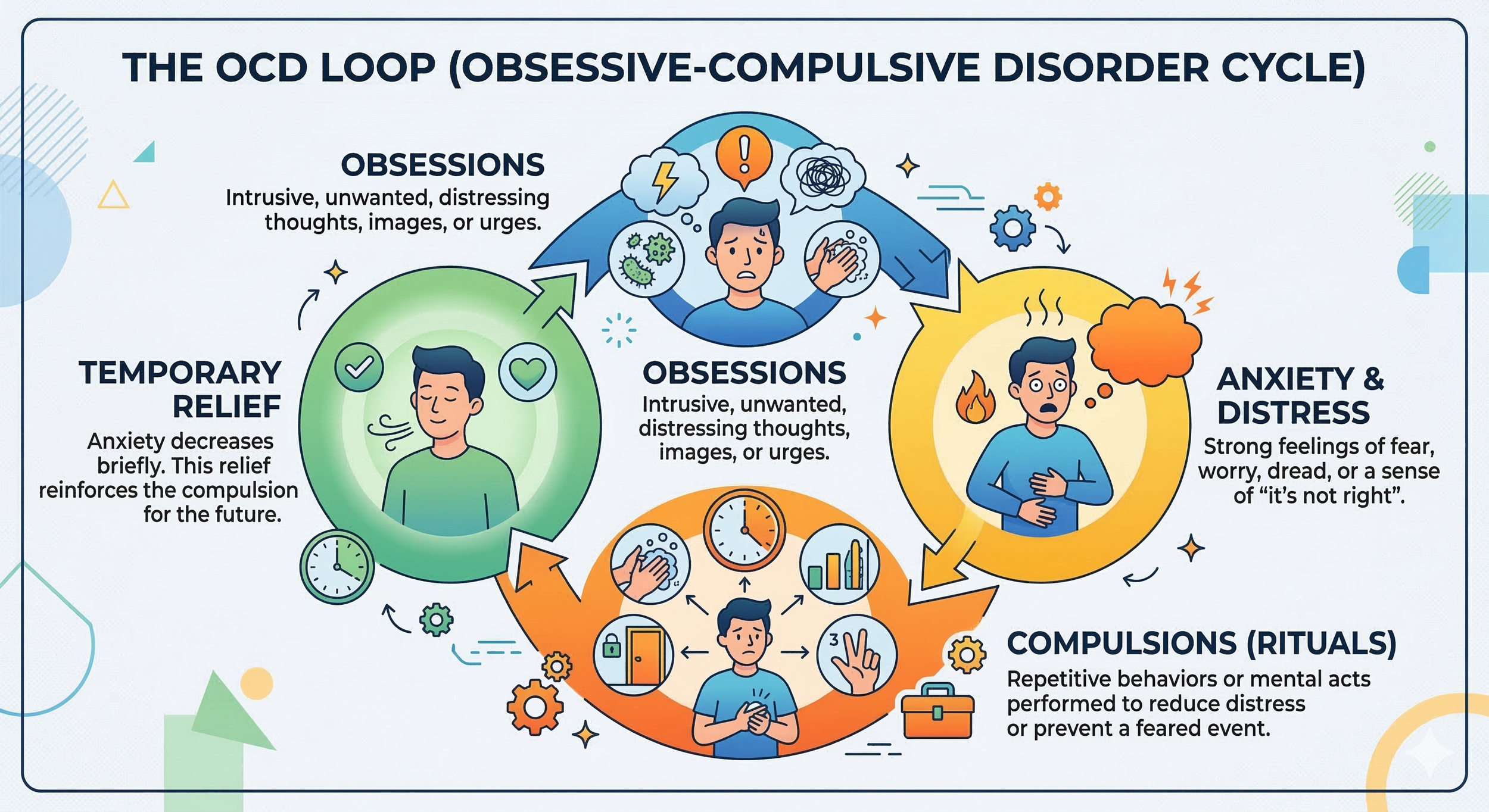
The OCD Cycle and Fertility
OCD thrives wherever certainty is impossible—and fertility is full of uncertainty.
Even with excellent medical care, perfect timing, and healthy reproductive systems, no one can guarantee a specific outcome. For someone vulnerable to OCD, that uncertainty can feel unbearable.
When applied to the reproductive journey, the OCD cycle typically looks like this:
1. The Obsession: An intrusive thought or image appears suddenly.
“What if I accidentally ruined my chances of getting pregnant this month?”
2. The Compulsion: To feel more certain, safe, or in control, you engage in a physical or mental behavior. You search online for hours, compare your experience to others on forums, analyze physical symptoms repeatedly, check fertility tracking apps over and over, or mentally review past decisions.
3. Temporary Relief: Your anxiety decreases briefly because you found a "reassuring" piece of data.
4. The Return of Doubt: A new "what-if" appears. “But what if that information was wrong? What if I misread the test?” And the loop starts all over again.
Unfortunately, every attempt to eliminate uncertainty accidentally teaches the brain that uncertainty is dangerous and must be solved immediately.
What Fertility OCD Can Look Like
Because fertility tracking is often medically recommended, it can be incredibly difficult to recognize when helpful monitoring has shifted into compulsive, anxiety-driven monitoring.
Hyper-Tracking
Tracking becomes difficult to stop even when it no longer feels useful. You may find yourself checking multiple apps, taking repeated ovulation tests long after your peak, recording every minor bodily sensation, and constantly comparing current and past cycles.
Somatic Hyperawareness
Your attention becomes glued to your body. Every cramp, twinge, headache, or wave of nausea feels potentially significant. You may spend large portions of the day trying to determine what these symptoms "mean" during the grueling two-week wait.
Reassurance Seeking
You repeatedly look for certainty from partners, friends, healthcare providers, online communities, fertility forums, and search engines. The reassurance helps briefly, but the relief never seems to last.
Mental Reviewing
You replay events repeatedly in your head: Did I time intercourse correctly? Did I eat something harmful? Did I exercise too much? Did I miss an important sign? Instead of creating clarity, this mental reviewing only creates more doubt.
Why "Just Relax" Doesn't Help
Women trying to conceive are frequently given well-intentioned but deeply frustrating advice: "Just stop thinking about it," "Relax and it will happen," or "Stress is probably making it harder."
While usually meant to be comforting, these comments can leave people feeling blamed and isolated. For someone struggling with anxiety or OCD, "just relax" simply creates another impossible task. Now there is a new fear: “What if my anxiety is the reason I’m not pregnant?”
The result is a cruel loop of anxiety about anxiety. No one can simply decide not to care about something deeply meaningful.
Fertility Challenges and Real Losses
It's also vital to acknowledge that fertility anxiety does not occur in a vacuum. Many women navigating these challenges have also experienced:
Failed fertility treatments (failed IUI or IVF cycles)
Reproductive trauma
In these situations, fears are not coming from nowhere. The goal of therapy is not to convince you that everything will be fine. The goal is to help you carry uncertainty, grief, fear, and hope without becoming trapped in endless, exhausting attempts to control what cannot be fully controlled.
Fertility OCD, Pregnancy OCD, and Postpartum OCD
One reason fertility OCD often goes unrecognized is that many people assume the symptoms will automatically disappear once pregnancy occurs. Sometimes they do—but often, the underlying themes simply shift.
The fear easily moves from "What if I can't get pregnant?" to "What if I harm this pregnancy?" and later, to postpartum intrusive thoughts like "What if I harm my baby?"
This is one reason specialized perinatal and postpartum mental health care can be so valuable. Understanding OCD across the reproductive journey allows treatment to address the underlying psychological process rather than only chasing the current, shifting fear.
Reclaiming Your Life While Trying to Conceive
The goal of therapy is not to stop caring about becoming pregnant. The goal is to stop allowing anxiety and OCD to take over your life while you wait.
With specialized, evidence-based treatment, many women learn how to:
Reduce compulsive tracking and checking behaviors
Respond differently to intrusive, sticky thoughts
Tolerate uncertainty without endless reassurance seeking
Stay anchored and present during the two-week wait
Separate their inherent worth from reproductive outcomes
Continue building a meaningful, vibrant life while pursuing parenthood
Trying to conceive is already hard enough. You shouldn't have to spend the process battling your own mind every day. If fertility anxiety or OCD has begun to consume your thoughts, relationships, or daily functioning, support is available. You do not have to navigate the uncertainty of this journey alone.
Not sure whether it's anxiety, OCD, or something else?
Many women assume their fertility worries are "just part of trying to conceive." A consultation with a therapist trained in perinatal mental health can help you better understand what you're experiencing and what treatment approach may be most helpful.
About the Author:
Dr. Erin Cook, PsyD, PMH-C is a licensed psychologist and Certified Perinatal Mental Health specialist at Red Elm Psychotherapy. Grounded in evidence-based care, her clinical practice includes helping individuals navigate anxiety, OCD, and complex transitions across the entire reproductive journey—from preconception and fertility challenges through pregnancy and the postpartum period.
Is ERP Hard? Why OCD Therapy Can Feel So Wrong at First
ERP can feel hard because it asks you to stop doing the very compulsions OCD says are keeping you safe. Here’s why ERP feels so wrong at first, what good treatment actually looks like, and why the discomfort can be part of recovery.
If the idea of Exposure and Response Prevention makes you want to close the browser tab, that makes sense.
ERP is considered a gold-standard treatment for OCD, but when you first hear what it involves, it can sound almost unreasonable: intentionally facing the thoughts, images, sensations, situations, or uncertainties that trigger anxiety while practicing not doing the compulsions OCD demands.
For many people, the first reaction is:
Absolutely not.
And honestly, that reaction is understandable.
If you are already exhausted by intrusive thoughts, panic, doubt, checking, reassurance-seeking, avoidance, mental review, or the constant need to feel certain, the idea of “facing the fear” may sound like the last thing you want to do.
So let’s answer the question directly.
Is ERP Hard?
Yes. ERP can be hard.
But ERP is not the introduction of fear into an otherwise peaceful life.
ERP is a way of bringing structure, support, and clinical direction to fear that is already running the show.
If you are new to ERP therapy, it helps to understand that the goal is not to eliminate fear immediately — it is to change how you respond to it.
Right now, OCD may already be making you face fear every day. It just does it without a plan. Alone. Urgently. At 2 a.m. In the middle of work. While you are trying to parent, sleep, pray, drive, love your partner, or live your life.
OCD says: Figure this out right now or something terrible might happen.
ERP says: We are going to stop letting OCD set the rules.
That is why ERP feels hard. Not because it is reckless. Not because your therapist is trying to scare you. But because ERP asks you to do the one thing OCD has trained you not to do:
Feel uncertainty without performing a compulsion to make it go away.
Why ERP Feels So Wrong at First
Most people with OCD are not short on insight.
You may already know the thought is irrational. You may know the fear is exaggerated. You may know that checking, Googling, confessing, replaying, or asking one more question probably will not give you lasting certainty.
Logic is not the problem.
The problem is that OCD does not feel like a logic problem. It feels like an emergency.
Your brain says:
Check one more time.
Ask one more person.
Replay it one more way.
Make sure you did not miss something.
Make sure you are not secretly dangerous, immoral, contaminated, irresponsible, unfaithful, sick, or wrong.
And when you do the compulsion, you may feel better for a moment.
That is the trap.
The anxiety drops. For a few minutes, it feels like you solved it.
Then the doubt comes back.
What if I missed something?
What if this time is different?
What if I am the exception?
That is the OCD cycle: obsession, compulsion, temporary relief, more doubt.
Every time you perform a compulsion to feel safe, you accidentally teach your brain that the alarm mattered. The compulsion works just long enough to make your brain ask for it again.
What ERP Actually Asks You To Do
ERP is not about proving that your fear is impossible.
That is usually what OCD wants: perfect certainty, perfect reassurance, perfect proof. A written guarantee from the universe.
ERP is different.
ERP asks you to practice a new response to fear.
That might mean letting an intrusive thought sit in your mind without trying to answer it. It might mean resisting the urge to check a lock, your body, your memory, your feelings, your intentions, or your symptoms. It might mean doing the thing OCD says you cannot do until you feel “sure enough.”
ERP can be used across many OCD themes, including contamination fears, harm-related intrusive thoughts, relationship doubts, religious or moral fears, and fears about identity, health, or responsibility.
In other words, ERP is not about feeling calm first.
It is about learning that you can move forward while anxiety is still there.
That is the part that feels so unnatural. OCD has trained your brain to believe that anxiety means stop. Analyze. Fix. Neutralize. Get certainty.
ERP helps you learn:
Anxiety is not always a stop sign.
A thought is not always a warning.
A feeling is not always evidence.
Uncertainty is not an emergency.
Good ERP Should Not Be Reckless
Because ERP has a reputation for being hard, many people worry that treatment will mean being thrown into their worst fear before they are ready.
That is not good ERP.
Good ERP is not punitive. It is not chaotic. It is not your therapist trying to overwhelm you to prove a point.
Good ERP is structured and collaborative. You and your therapist identify the OCD cycle, name the compulsions, and build a plan. You start with exposures that are challenging but workable. You learn how to face discomfort without giving OCD the response it demands.
The goal is not to be fearless.
The goal is to stop treating fear like it gets to make all your decisions.
Will ERP Make My Anxiety Worse?
At first, ERP can make anxiety louder.
That does not necessarily mean something is going wrong. It often means you are doing something very different from what OCD expects.
When you stop doing compulsions, your brain may protest. It may tell you that you are being careless. Irresponsible. Dangerous. It may tell you that you are ignoring something important.
This is one of the hardest parts of ERP:
Doing the work can feel wrong before it feels freeing.
But that feeling is not proof that you are in danger. It is often the feeling of your brain learning a new pattern.
For years, your nervous system may have treated uncertainty as an emergency. ERP gives it a different lesson:
I can feel anxiety, doubt, or uncertainty without obeying OCD.
Is ERP Worth It?
ERP is hard.
But untreated OCD is also hard.
OCD can shrink your world quietly. It can take over your mornings, your relationships, your work, your faith, your body, your parenting, your memories, and your sense of self. It can make you spend hours trying to feel certain and still leave you doubting five minutes later.
ERP gives you a different path.
Not a magic switch.
Not instant certainty.
Not a promise that you will never have an intrusive thought again.
But a structured way to stop organizing your life around fear.
ERP is hard because it asks you to stop playing by OCD’s rules.
And that is also why it works.
OCD Therapy in Virginia
At Red Elm Psychotherapy, we provide specialized OCD therapy using Exposure and Response Prevention for adults in Virginia. We help clients understand their OCD cycle, reduce compulsions, and build a more flexible relationship with uncertainty.
If ERP feels intimidating, that does not mean you are not ready. It means you understand what OCD has been asking of you.
You do not have to face it alone or without a roadmap.
Schedule a consultation today.
About the Author
Dr. Niles Cook is a clinical psychologist specializing in OCD and anxiety disorders, with advanced training in Exposure and Response Prevention. At Red Elm Psychotherapy, he helps adults across Virginia understand their OCD cycle, reduce compulsions, and build a more flexible relationship with fear, doubt, and uncertainty.

When Insight Isn’t Enough: Why OCD Still Feels So Convincing
You know the thought is irrational, yet five minutes later you're back in the loop. The problem isn't a lack of logic—it’s an excess of it. Discover why your intelligence is being weaponized against you and how to finally 'drop the rope' in the mental tug-of-war.
You know the thought doesn’t make sense. You’ve analyzed it from every angle. You’ve checked the facts. You’ve reassured yourself.
Maybe you’ve even had a moment where you thought: “Okay. This is definitely Obsessive-Compulsive Disorder (OCD).”
And then five minutes later, the anxiety comes rushing back. Your stomach drops. The doubt feels real again. And suddenly you’re back in the loop trying to solve it one more time.
If this happens to you, you are not failing at being rational. In fact, many people with OCD are exceptionally intelligent, analytical people. That’s part of what makes OCD so convincing.
OCD Turns Intelligence Against You
In most areas of life, thinking harder helps. Being responsible and paying attention to details are traits that probably helped you succeed in school, work, or parenting.
But OCD hijacks those same strengths. Instead of using your mind to solve real-world problems, OCD pulls you into impossible ones:
“What if I secretly meant that thought?”
“What if I’m missing something important?”
“What if I can never be fully certain?”
At some point, the thinking itself becomes the compulsion. Not because you’re irrational, but because your brain is desperately trying to make the anxiety stop.
What Mental Compulsions Actually Look Like
A lot of people imagine OCD as visible checking or hand washing. But many compulsions happen entirely inside your head. From the outside, you may look calm. Inside, you are exhausted.
You might spend hours replaying conversations, reviewing memories, or checking whether a feeling "feels true." Depending on what you value most, these loops can take many forms:
Relationship OCD (ROCD): Constantly analyzing your partner or your feelings to "prove" you are in the right relationship.
Perinatal OCD: Intrusive, terrifying thoughts about the safety of your baby and the constant mental checking that follows.
Scrupulosity: A painful loop of moral or religious doubt, where you feel you must constantly "fix" your standing with God or your conscience.
The OCD Cycle: The universal engine that keeps all these themes running on a loop.
Why Insight Alone Doesn’t Stop OCD
One of the most painful parts of OCD is that you likely already know your fears are irrational. Insight is not the problem. You can understand OCD intellectually and still feel trapped by it emotionally because OCD is not a logic problem; it’s an alarm system problem. Your brain sends out a false signal of danger, and your mind works overtime to explain why the danger feels so real. Unfortunately, the more seriously you treat the thought—by analyzing or researching it—the more important your brain believes it must be.
The Tug of War
Imagine you are standing at the edge of a canyon. On the other side is a monster representing your intrusive thoughts. Between you is a rope.
The moment an intrusive thought appears, the monster yanks the rope. Instinctively, you pull back. You try to prove the thought wrong or get certainty. But the harder you pull, the more consumed you become by the fight. Soon, your entire life revolves around the rope.
ERP Is About Leaving the Fight
This is where Exposure and Response Prevention (ERP) changes things. ERP is not about proving the intrusive thought false or "thinking more rationally."
ERP helps you learn how to stop engaging with the struggle altogether. Whether you are dealing with harm OCD, contamination fears, or the constant "background noise" of uncertainty, the goal is not to defeat the monster; the goal is to stop organizing your life around it.
What “Dropping the Rope” Looks Like:
ERP teaches you to practice allowing uncertainty to exist.
That might mean:
Allowing a scary thought to stay without analyzing it.
Resisting the urge to mentally review your day.
Noticing anxiety without trying to "neutralize" it.
At first, this feels deeply uncomfortable. It feels irresponsible to let the "what if" go unanswered. But over time, your brain learns the truth: The thought itself was never the danger.
Here is the problem with doing this alone: Your brain is convinced that the rope is the only thing keeping you safe. It tells you that if you let go, the monster wins, or something terrible will happen. Dropping the rope feels like an act of negligence.
This is one of my main roles in guiding clients through [Exposure and Response Prevention (ERP)]: to stand at the edge of that canyon with you. I help you tolerate the "itch" to pull back until your brain finally learns that the monster can’t actually cross the canyon—whether you hold the rope or not.
A 30-Second Exercise: Practice the Pause
You don’t have to drop the rope forever right this second. Today, just practice delaying the pull.
Next time you feel that jolt of anxiety and the urge to "figure it out" or check a memory hits:
Acknowledge the rope: Say to yourself, "OCD just threw me the rope."
Set a timer for 30 seconds: Do not analyze, do not Google, and do not replay the memory for just thirty seconds.
Feel the tension: Notice the discomfort in your body without trying to fix it.
Even if you go back to the loop after those 30 seconds, you’ve just proven something huge: You are the one in control of your hands, even when the anxiety is loud.
You Don’t Need More Insight. You Need a Different Response.
Many people who reach out for OCD treatment are already highly self-aware. They’ve read the articles; they can explain the cycle better than anyone. But they still feel trapped.
Recovery doesn't happen through more analysis. It happens through learning a different relationship with fear.
OCD Therapy in Virginia
I work with adults struggling with OCD, intrusive thoughts, rumination, and mental compulsions using evidence-based ERP therapy.
Together, we focus on helping you step out of the exhausting mental loops so you can spend less time trapped in your head and more time fully engaged in your life.
Ready to drop the rope?
About the Author
Dr. Niles Cook is a licensed clinical psychologist and co-founder of Red Elm Psychotherapy. He specializes in helping high-achieving adults and professionals who are exhausted by the "intelligence trap"—where the same analytical skills that made them successful are now being used by OCD to keep them stuck in cycles of doubt.
Using Exposure and Response Prevention (ERP), Dr. Cook provides a structured, no-nonsense path for clients to stop over-analyzing their lives and start living them. His approach is direct, collaborative, and designed for those who need more than just insight—they need a different way to respond to fear.
Dr. Cook provides specialized telehealth therapy across the state of Virginia.
Note: This content is educational and does not constitute medical advice or a therapist-client relationship. If you are in a crisis, please call 988 or go to the nearest emergency room.

Why Your Relationship Feels Different After a Baby — Especially When Anxiety or OCD Is Involved
Some couples don’t fight more after a baby.
Instead, things start to feel… off.
You’re functioning. You’re getting through the day. But something in the relationship feels quieter, more distant—and harder to explain.
For many high-functioning women, anxiety and intrusive thoughts don’t just stay internal. They subtly reshape how you show up with your partner.
Some couples don’t fight more after they bring their baby home. They aren’t having dramatic arguments or obvious problems. But somewhere between the diapers and the sleepless nights, something shifts.
Things don’t feel bad—just… off.
There’s a little more distance. A little less ease. You might find yourself feeling less connected to the person you just started a family with—and you aren't entirely sure why.
For many women, this shift is compounded by anxiety, intrusive thoughts, or patterns that feel difficult to explain—especially during pregnancy or the postpartum period. If you’re having thoughts that feel disturbing, out of character, or hard to talk about—you are not alone. This is something we treat often at Red Elm Psychotherapy.
When Anxiety Becomes a Third Partner
When anxiety or OCD is present, the relationship often becomes one of the primary places it gets expressed. This can show up as general anxiety, intrusive thoughts, or more defined OCD patterns—but the impact on the relationship often feels the same.
Anxiety is driven by a need for certainty. In a partnership, that often translates into:
Constant Scanning: Checking your partner’s face or tone for signs of frustration, boredom, or distance.
Reassurance Seeking: Asking the same questions repeatedly to soothe a “sticky” thought (e.g.,“Is the baby breathing?” or "Are we okay?" ).
Over-Responsibility: Feeling like you must carry the entire emotional or physical load to prevent something “bad” from happening.
Hypersensitivity: Interpreting a neutral moment—like a quiet dinner or a short text—as a sign that the relationship is failing.
These thoughts are unwanted, distressing, and often completely out of character. They are not a reflection of your intentions or the quality of your bond. We go into more detail about how this pattern works on our Perinatal OCD page.
Sometimes, the anxiety begins to focus on the relationship itself. This is often referred to as Relationship OCD (ROCD), where “sticky” thoughts lead you to constantly question your partner’s “rightness” or search for flaws as a way to reach a certainty that doesn’t exist.
The Reassurance Loop: The Unwitting Accomplice
In high-functioning couples, partners are often incredibly kind and helpful. However, that kindness can unintentionally feed the anxiety.
In the world of OCD, this is called accommodation—when a partner’s well-intentioned efforts to reduce your distress actually keep the anxiety cycle spinning. Many people feel ashamed of how much reassurance they need and worry about "burdening" their partner.
A partner may provide reassurance, engage in repetitive “what-if” conversations, or try to become the "solution" to intrusive thoughts. The relationship starts to function as a tool for resolving anxiety. It works briefly, but the relief never lasts. Over time, this creates a painful cycle of tension, resentment, and loneliness—even when you’re sitting right next to each other.
The High-Functioning Mask
For many of the couples we see in Vienna and across Northern Virginia, everything looks fine from the outside. You are showing up. You look responsible. You are getting the job done.
You may be caring for a baby, managing a household, or returning to work—all while internally feeling overwhelmed or disconnected. But behind closed doors, there can be a deep sense of isolation. You aren’t “bad at communicating”—you’re navigating a system under sustained strain.
It’s Not Broken—It’s Under Strain
If this feels familiar, it doesn’t mean you picked the wrong partner or that your relationship is broken. It often means your relationship has been pulled into a cycle of anxiety.
The solution isn’t simply to “communicate better.” It’s understanding how you relate to each other through the lens of anxiety—and how certain patterns, even the ones born out of love, can keep both of you stuck.
How Therapy Helps
Therapy can help separate the anxiety from the relationship. Through structured, evidence-based approaches—including Exposure and Response Prevention (ERP) when appropriate—treatment focuses on:
Separating the anxiety from the person: Understanding that intrusive thoughts are not a reflection of who you are.
Reducing reassurance loops: Learning how to support each other without reinforcing the cycle.
Rebuilding steadiness: Moving away from reactive patterns and back toward the values that brought you together.
You don’t have to keep feeling "off." Understanding the pattern is often the first step toward feeling more like yourselves again.
Ready to Take the Next Step?
If your anxiety feels constant, intrusive, or difficult to step out of—especially during pregnancy or after having a baby—it may be more than something to simply "push through."
We specialize in helping women navigate postpartum anxiety, intrusive thoughts, and OCD. We use structured, evidence-based treatment designed to help you step out of the loop and feel more like yourself again.
We offer in-person sessions in Vienna, VA and work with clients across Virginia via telehealth, including McLean, Arlington, and the surrounding Northern Virginia area.
About the Author
Dr. Erin Cook, PsyD is a licensed clinical psychologist and co-founder of Red Elm Psychotherapy, a Virginia-based practice specializing in perinatal mental health and OCD. She works with women navigating pregnancy, postpartum, and early motherhood—particularly when anxiety or intrusive thoughts feel overwhelming or out of character.

Relationship OCD: Why You Can’t Stop Doubting Your Relationship
Relationship OCD can make normal doubt feel urgent, dangerous, and impossible to let go of. Learn how ROCD traps you in checking, comparison, reassurance-seeking, and “what if” loops — and how ERP therapy can help.
“What if I don’t actually love them?”
“What if I’m making a huge mistake?”
“Why am I constantly overanalyzing every single thing they say or do?”
Most people experience moments of doubt in a relationship. But for some, these questions don’t just pass—they loop. They intensify. They become a background noise that never truly shuts off, eventually taking over your daily life and your ability to enjoy your partner.
If your relationship feels less like a partnership and more like a puzzle you are desperately trying to "solve," you might be experiencing Relationship OCD (ROCD).
What Is Relationship OCD?
ROCD is a common subtype of Obsessive-Compulsive Disorder. It isn’t a sign that your relationship is "wrong" or that you’ve fallen out of love. Instead, it is a cycle driven by a low tolerance for uncertainty.
While everyone has fleeting doubts, someone with ROCD feels an urgent, crushing need for 100% certainty about their feelings, their partner’s flaws, or their long-term compatibility. Because perfect certainty is impossible to find, the brain stays stuck in a loop of searching for it.
Common Signs of ROCD
ROCD usually manifests through intrusive thoughts (obsessions) and the actions you take to quiet them (compulsions). You might find yourself:
Mentally Checking: Constantly asking yourself, "Do I feel 'the spark' right now?" while kissing or hanging out.
Comparing: Obsessively comparing your partner’s traits or your relationship to friends, exes, or even fictional characters.
Reassurance Seeking: Asking friends, family, or even your partner if you "seem" happy or if the relationship looks "right" to them.
Researching: Spending hours on forums or reading articles trying to find a definitive "sign" that you should stay or leave.
Hyper-fixating on Flaws: Becoming consumed by a partner’s physical "imperfections" or minor personality quirks as evidence that they aren't "The One."
Why It Feels So Real
The paradox of OCD is that it targets what you value most. If you didn’t care about your partner or the concept of love, your brain wouldn't bother using these thoughts to scare you.
Furthermore, ROCD exploits the fact that human emotions are naturally fluid. We don’t feel "madly in love" every second of every day. To an ROCD brain, a slight dip in affection isn't just a normal part of a Tuesday—it’s viewed as an emergency that must be analyzed immediately.
ROCD vs. Normal Doubt
How do you know if you're in the wrong relationship or if you just have OCD?
Normal Doubt
Comes and goes; usually triggered by specific, real-world issues.
Doesn't usually result in hours of "mental work" or research.
You can focus on other parts of your life (work, hobbies).
Feelings are generally stable despite the doubt.
Relationship OCD
Persistent, intrusive, and urgent.
Leads to repetitive compulsions to ease anxiety.
The doubt feels like a "cloud" over everything you do.
Feelings feel "gone" because anxiety is suppressing them.
The Cycle of ROCD
ROCD thrives on a specific loop:
The Trigger: A thought or feeling (e.g., “I didn’t miss them today”).
Anxiety: A spike of fear or "urgency" to figure out what that means.
Compulsion: You Google "signs of falling out of love" or check your feelings.
Temporary Relief: You feel better for a moment because you found an answer.
The Repeat: The doubt returns, and you need a stronger "fix."
There is a Way Out
The goal of therapy isn't to prove that your relationship is perfect—it’s to help you live comfortably with the fact that no relationship is certain.
Exposure and Response Prevention (ERP) is the gold standard for treating ROCD. It helps you break the cycle by teaching your brain that you don't have to "answer" every intrusive thought that pops into your head. You can learn to experience a doubt without letting it dictate your actions.
You don’t need to end your relationship to get relief, and you don’t need to reach 100% certainty before you start feeling better.
Take the Next Step
If this cycle feels familiar, you don’t have to keep trying to figure it out on your own. Our specialists are trained in evidence-based tools to help you reclaim your life from the "What Ifs."
Explore our Relationship OCD Service Page
Learn more about OCD Therapy
HowERP Therapyworks
You deserve to be present in your life, rather than stuck in your head.
About the Author
Dr. Niles Cook, PsyD is a licensed clinical psychologist and co-founder of Red Elm Psychotherapy. He specializes in the treatment of obsessive-compulsive disorder (OCD) and anxiety using Exposure and Response Prevention (ERP). Dr. Cook works with high-achieving adults and professionals who feel stuck in cycles of overthinking, doubt, and perfectionism. He provides telehealth therapy across Virginia. He is listed with the International OCD Foundation.